Seminar
Depression
Gin S Malhi, Erica Bell, Anna Stavdal, Chia-Yi Wu, Anne Naylor, Veena Kumari
- Summary
- Introduction
- Epidemiology
- Causes and mechanisms
- Diagnosis
- Managing depression
- Conclusion
- Panel 1 から Panel 9 まで
- Panel 1: Depression vulnerability factors
- Panel 2: Watchful waiting in primary care
- Panel 3: Mood monitoring
- Panel 4: Suicidal thoughts and risk of suicide
- Panel 5: Risky lifestyle habits
- Panel 6: Sleep pharmacotherapy
- Panel 7: Risk of suicide and antidepressants
- Panel 8: Antidepressant discontinuation syndrome
- Panel 9: Complementary treatments and emerging therapies
- 1ページ目「Search strategy and selection criteria」
- References
- Fig1
- Fig2
- Table1
- Fig3
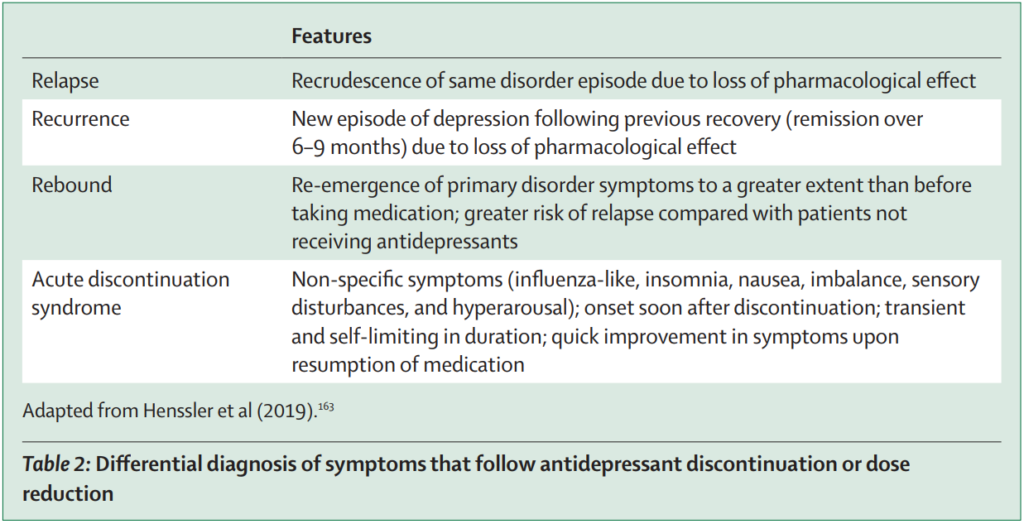
- Table2
- Table3
Summary
Depression is a common illness that affects people within every society around the world. It afflicts the young and the old and everyone in between, and as such poses an immense global burden. New interventions and a deeper understanding of this illness are emerging, but improving the use of existing treatments is equally important and might be a more efficient and effective strategy to addressing depression. Therefore, it is imperative that we improve the diagnosis of depression and its clinical management.
Introduction
Depression affects approximately a quarter of a billion people globally, of all ages and from all walks of life. In this Seminar, we focus on depression in adults, which causes functional impairment, affects relationships and work, and is costly to the individual and society as a whole. The psychosocial impact of this profoundly stigmatising illness is deep and simultaneously far-reaching.
Epidemiology
Prevalence
The global prevalence of depression varies, with socioeconomic and cultural factors, as well as stigma, playing a substantial role. Absolute case numbers and rates of depression continue to increase, and depression globally is greater in women than in men (2:1), with the gender gap remaining relatively consistent throughout adulthood following puberty—a difference attributed in part to differential hormonal and developmental changes.
Depression typically begins in the second decade of life, with nearly 40% of people with depression having their first episode before age 25 years. By its nature, it is recurrent and nearly a quarter of people will have a further episode within 5 years of onset, and the likelihood of additional episodes increases once recurrence is established. In general, one in 15 adults have depression in any year and a fifth of people experience depression in their life; however, the true rates of depression are probably higher.
Course and prognosis
In community settings, most depressive episodes remit after 2–6 months and resolve within a year, but in primary and secondary care settings, between a third and a half of patients remain unwell for more than a year, and most patients have further episodes, with a recurrent pattern more likely in patients with early onset.
Causes and mechanisms
Research examining the precursors, onset, and response to treatment of depression has identified probable causal factors and mechanisms.
Contemporary concepts of depression draw on diverse molecular, genetic, psychological, and social mechanisms, but none of these concepts fully explain the illness satisfactorily. New neuroscientific and psychological models implicate neural networks, cardiovascular systems, neuroendocrine systems, and the gut microbiome. In addition, inflammation caused by stress creates so-called scars of depression in both bodily and brain systems.
In this Seminar, we focus on our current understanding of depression based on the diathesis-stress model, which is used to inform clinical diagnosis and management and helps provide patients with meaningful causal explanations. The diathesis-stress model suggests that depression might be caused by a combination of a stressful event and individual vulnerability. Furthermore, this model serves as a useful schema for the multitude of depression-related factors that emerge from biological, psychological, and social determinants.
Diagnosis
Screening and detection
Distress caused by depression prompts individuals to seek help, and informal assistance from friends and family, and searching the internet for solutions, which are usually sought before consulting a professional. In part, such delays also occur due to the stigma associated with mental illness and difficulties accessing care. Consequently, weeks or months might pass before individuals receive professional help, and often individuals are not properly diagnosed for years after initially seeking help.
Greater depression awareness and access to screening have increased presentations and treatment uptake. However, the use of screening tools alone can both fail to detect serious illness and overdiagnose depression, leading to mistreatment. Therefore, screening alongside clinical evaluation is optimal, and hence screening measures are increasingly being used in primary care to inform medical consultations; in practice, simply asking about two symptoms over the past 2 weeks, as per the Patient Health Questionnaire-2, can be sufficient for detecting depression.
Diagnosing depression
The major taxonomies (ICD and Diagnostic and Statistical Manual of Mental Disorders [DSM]) provide standardised diagnoses for depressive disorder (ICD-11) and major depressive disorder (DSM-5-TR; for descriptions of additional depressive disorders, see the appendix). These descriptors refer to the entirety of the illness over the course of a person’s lifetime and should not be confused with depressive episodes, which are acute exacerbations. The principal features of depression are low mood and anhedonia (an inability to gain pleasure from activities the person usually finds enjoyable); in total, the person must have a minimum of five symptoms occurring most of the time and for at least a fortnight, with the number of symptoms broadly reflecting illness severity and causing functional impairment. However, before making a definitive diagnosis of depression, it can be useful to assign a provisional diagnosis.
In practice, the diagnosis of depression usually starts as a clinical suspicion that is confirmed or refuted by further questioning. A family history of depression or recent life events provide additional clues that can help make a provisional diagnosis, but due to limited consultation time or because the illness is still evolving, these factors might be all that is possible during the initial stages of presentation. If depression is suspected, another appointment should be scheduled and the patient should be asked to monitor their mood, sleep, and activities in the interim. If possible, partners, family, and carers should be recruited as they can corroborate information and their engagement helps validate the patient’s distress.
Clinically, diagnosing depression involves eliciting key symptoms and determining their impact on an individual’s life, as well as charting their pattern over time to map the course of the illness. In practice, patients seldom present spontaneously with low mood or sadness, and instead usually complain about general distress, sleep disturbances, pain, and fatigue. Therefore, it is useful to have in mind depression as a potential diagnosis and routinely ask about its key symptoms, and if depressive symptoms are identified, to gauge their severity and the functional impairment that they cause, as this informs diagnosis and management.
Together, the number of symptoms, their severity, and the functional impairment that they cause provides a measure of the overall severity of a depressive episode, which can be broadly categorised as less severe or more severe. Describing depression in this manner allows treatment to be informed by recommendations made by various guidelines, particularly those made by the UK National Institute for Health and Care Excellence.
Sometimes a diagnosis cannot be made immediately in clinical practice, and appraising the patient over a short period of time is useful—a process called watchful waiting. During this time, mood monitoring can be commenced, and this might also help with diagnosis and assist with subsequent tracking of any treatment response. Digital health technologies are especially useful in this regard as they signal to the patient that a proactive approach has been adopted. Receiving a diagnosis of depression and starting treatment are inherently stressful, and commencing antidepressant treatment can occasionally increase the risk of self-harm. Therefore, the diagnosis and management of depression should be fully explained to the patient from the outset, and the probable prognosis and potential adverse effects of treatment should be discussed.
Managing depression
Planning and implementing treatment
Treatment can be planned once the symptom profile and severity of depression have been characterised. First, the patient’s experience and treatment preferences should be considered within the context of practical limitations such as treatment availability, access, and cost. When possible, treatment choice should be evidence-based and draw upon expertise, and treatment options should be aligned with clinical features of the illness while considering patient characteristics such as age, gender, and individual circumstances.
The initial goal of treatment is to relieve distress and achieve remission. Once depressive symptoms subside, the subsequent aim is recovery, after which the emphasis shifts to preventing recurrence. Successful treatment of depression often requires a combination of interventions, which can be administered concurrently and sequentially; a multifaceted strategy should be used whenever possible and individual interventions should be selected with a view to maintaining them. The settings in which treatment will be administered, and by whom, should be considered, and if a specialist (eg, a psychiatrist or psychologist) will be needed, then prompt referral and engagement should be considered from the outset of management.
Once management is under way, the individual’s clinical symptoms should be continually reassessed and treatment tailored accordingly. In practice, this involves confirming the diagnosis and assessing treatment response at every clinical encounter, especially when making changes to treatment. Concurrent life stressors can exacerbate depression, and it is important to know about an individual’s supports and any obligations they might have (eg, working or caregiving responsibilities). Careful monitoring is important because comorbid psychiatric illnesses such as substance use or anxiety disorders are common and can complicate treatment, and also because depressive episodes might represent an emerging bipolar disorder, which only becomes evident once mania manifests.
Most cases of depression can be treated successfully using four broadly complementary therapeutic strategies: psychoeducation, lifestyle modifications, psychological interventions, and pharmacotherapy. A fifth strategy is physical treatments (eg, electroconvulsive therapy and other neuromodulators), which are mostly used to treat severe depression that has not responded to other treatments or requires hospital admission for specialist management. However, since physical treatments are used less often than the other strategies, they are not discussed in this Seminar. In contrast, psychoeducation is integral to the management of depression and should be instituted from the outset.
Psychoeducation
Generally, psychoeducation involves providing knowledge and instruction about an illness and its management in an unstructured or formal manner to the patient and their carers. Evidence for psychoeducation in the prevention and treatment of clinical depression is scarce, but it has been shown to benefit those with chronic diseases. It also informs patients’ expectations and helps them accept that they have a chronic condition. In addition, psychoeducation enhances doctor–patient engagement and therapeutic adherence, while also instructing patients on how to monitor their illness. Therefore, whenever a suitable opportunity arises, clinicians should educate patients about the likely causes and clinical symptoms of depression, and its treatment and prognosis.
Lifestyle modifications
In depression, healthy lifestyle factors (eg, diet, exercise, and sleep) and risky lifestyle habits (eg, smoking tobacco, drinking alcohol, and using substances) have been shown to play an influential role. Therefore, alongside modifiable healthy lifestyle factors, risky lifestyle habits commonly associated with depression (in particular smoking and drinking, which are amenable to change albeit with greater difficulty) should also be addressed.
Healthy lifestyle factors
Balanced diet, regular exercise, and proper sleep prevent or at least delay the onset of depression. Furthermore, diet, exercise, and sleep are inherently entwined such that change in one affects the other two, hence their grouping as healthy lifestyle factors. Each factor has a biological and psychological component, and in practice, the most common problem is their disruption, which can lead to depression or exacerbation of existing symptoms.
Exercise
International guidelines recommend exercise to treat the symptoms of less severe depression and improve sleep quality and cognitive function. This recommendation is supported by meta-analyses of controlled treatment studies in adults with depression that show that exercise produces tangible benefits with an overall moderately large effect size. Research examining the benefits of various types of exercise in adults with depression highlights some specificity according to age and gender. For instance, aerobic exercise, walking, and jogging, as well as strength exercises and yoga, are on par in terms of efficacy with cognitive behavioural therapy (CBT), and evidence for each of these activities is strong, positioning them as more effective than selective serotonin reuptake inhibitors (SSRIs). Furthermore, although there is no clear age or gender specificity for general exercise (eg, walking, jogging, and aerobic exercise), strength exercises produce greater improvements in younger adults and women. Conversely, yoga is of greater benefit to men and older individuals. The reasons for certain exercises being efficacious are multifaceted and might include other factors such as social interaction and skill acquisition. Additionally, exercise is more beneficial when structured (time of day and frequency) and undertaken in combination with psychological interventions and medications (eg, SSRIs) and its benefits extend into old age. Thus, in addition to its general health benefits, exercise is particularly useful in the treatment of depression as it alleviates symptoms and can prevent onset and recurrence.
Diet
Growing interest in whether modifying diet can treat and perhaps prevent depression has led to increasing calls for clinicians to be aware of the potential benefits of different types of diet and to play a role in implementing dietary change. The links between diet and depression are less direct than those found in other illnesses such as diabetes, but gut microorganisms, stress hormones, and brain neurotrophins have all been shown to actively affect the immune, inflammatory, and hypothalamic–pituitary axes in depression. Nevertheless, specific dietary excesses and deficiencies that predictably lead to depression are yet to be determined, and the main benefit of certain diets seems to be the prevention of depression, possibly by reducing inflammation.
Recent research studies examining the relationship between diet, mood, and the gut microbiome have yielded new insights. However, more research is needed before specific recommendations can be made to predictably alter mood through changes to the gut microbiome, especially as most findings are based on animal studies and human dietary patterns vary considerably. Furthermore, the properties of ingested food are relatively distal to putative mood effects within the brain. Nonetheless, a Mediterranean diet significantly benefits mood and diminishes the risk of depression, possibly because it contains healthy food groups and has a low inflammatory index.
Studies examining specific foods from a broad range of food groups have also found similar but modest benefits that require replication. Conversely, ingesting excessive ultra-processed foods and refined sugars and having a proinflammatory diet increases the likelihood of depression. Therefore, a balanced, healthy diet containing Mediterranean diet food groups could benefit mood in people with depression.
Sleep
In depression, patients often have disturbed sleep (sleep dysfunction), which they describe as difficulty sleeping (insomnia) and waking too early (early morning waking), which typically manifest as too little sleep (reduced duration) and poor-quality sleep (lack of slow-wave sleep). Sleep problems such as these can be addressed using medications but are initially best managed using non-pharmacological interventions.
Establishing good sleep hygiene by modifying lifestyle habits and improving exercise and diet is important initially. CBT, which addresses anxiety and negative cognitions, is the most effective strategy for improving sleep, although exercise is also beneficial, especially in combination with other interventions. Bright-light therapy, which acts via the suprachiasmatic nucleus, might also be beneficial, especially for subjective sleep quality, but the effect is stronger in combination with antidepressants and particularly in seasonal depression.
Other psychological strategies (eg, meditation techniques such as mindfulness and body scanning) and physical interventions (eg, hypothermic bathing and acupuncture) appear to do no harm, but they do not seem to be particularly beneficial either. Therefore, despite multiple options for modifying sleep without needing medication, there is only strong evidence for CBT and exercise to date, and in individuals with either seasonal depression or depression with substantial phase-shifting of sleep, bright-light therapy might provide some modest benefit.
If non-pharmacological approaches for sleep dysfunction are ineffective then pharmacological treatments for sleep can be considered.
Psychological interventions
Most patients favour psychological interventions to address their depression; psychotherapeutic approaches inherently create a therapeutic relationship that increases treatment satisfaction and adherence. This therapeutic bond plays an important role when combining psychological interventions with other treatments, and in practice, although psychological interventions have an independent effect, combination therapy is more effective than individual therapies.
General principles
When choosing a psychological approach, the psychological symptoms, severity of depression, and individual characteristics of a patient that might influence their treatment response should be considered. Common psychological targets include negative cognitions and interpersonal issues. Regarding severity, grading depression as less or more severe can be useful, but more granular gradation does not further inform treatment choice.
Efficacy of psychological interventions
CBT, interpersonal therapy, behavioural activation therapy, problem-solving therapy, and mindfulness-based therapies, as well as short-term psychodynamic psychotherapy, all benefit patients with depression. Of these, CBT is the best researched and most widely available, and although particular therapies conceivably engage specific psychological targets, there is insufficient evidence to show significant differences in efficacy between the various approaches. One reason why differentiation of psychological therapies in terms of efficacy is difficult is that they all share some elements. Their effects on depressive symptoms are also thought to be mediated by shared cognitive mechanisms (eg, change in dysfunctional attitudes for both CBT and interpersonal therapy). However, some therapy-specific mechanisms could also play a role (eg, change in experiential avoidance for acceptance and commitment therapy but not for CBT or interpersonal therapy). Hence, the neural mechanisms implicated in the psychological effects of these interventions appear to overlap (eg, top-down modulation reducing dysfunctional thought processes), while some networks seem therapy-specific. Therefore, tailoring psychological interventions in practice is useful, as well as targeting specific symptoms so that therapy is structured and meaningful.
In addition to the benefits of acute treatment, considerable evidence points to the efficacy of psychological interventions in relapse prevention, with ongoing psychological engagement helping prevent future depressive episodes and enabling prompt intervention. Furthermore, psychological interventions have also been shown to be effective for individuals who have partially remitted, with therapy reducing residual symptomatology and the risk of relapse across a broad range of patient characteristics and treatments.
Regardless of illness severity, psychological therapies delivered in one-to-one or group settings, and when administered in combination with medications, are better than treatment as usual. In community care, treatment as usual might involve psychoeducation or antidepressant medication, or both. However, based on the effect sizes observed across studies, CBT and behavioural activation therapy appear to produce greater symptom reduction when delivered in a group setting than one-to-one sessions in less severe depression, whereas one-to-one sessions are more effective than group therapy in more severe depression. Nevertheless, in-person individual therapy is regarded as the gold standard of psychological interventions in practice, even though there is insufficient access to individual CBT in many settings around the world due to scarce availability and high cost. Consequently, alternative settings and means of delivery such as group and internet-based therapy are popular, and in many cases these more cost-effective and accessible options appear to be equally effective. Indeed, the greater effectiveness of CBT is clearly evident when compared with long-term pharmacotherapy.
Digital health technologies for psychological interventions
The uptake of digital health technologies has increased in recent times because they can be accessed independently without necessarily relying on support from others (ie, they can be unguided, self-directed, or guided or facilitated).
In guided programmes, the facilitator might have clinical expertise and help drive engagement, which can either be delivered live (synchronous; occurring at the time the individual is engaging with digital health technologies) or delivered later (asynchronous). Generally, guided digital health technologies have been found to be more effective than those that are self-directed, and internet CBT (i-CBT) produces significant effect sizes when guided, with benefits persisting beyond 12 months.
When considering severity in less severe depression, i-CBT shows greater benefits than treatment as usual or waiting list, with emerging evidence that text-delivered CBT is also an effective option. In more severe depression, guided i-CBT seems to produce larger symptom reduction compared with non-guided i-CBT. Notably, there is no significant difference between guided and unguided i-CBT for less severe depression. Therefore, i-CBT is recommended as a first-line monotherapy for less severe depression and adjunctive use is recommended for more severe depression, with guided therapy being preferable for more severe depression.
However, irrespective of the severity of depression, the scalability and low-resource implication of i-CBT make it ideal for use with or without guidance and support, and it is especially helpful in settings where there is high demand and long waiting times, or where there are barriers to accessing outpatient services. Furthermore, i-CBT is well received in terms of patient satisfaction and achieves good clinical outcomes, although the real-world effectiveness of these results is difficult to parse due to the challenge of generalising findings from clinical trials to the general population. Although i-CBT has received ample attention, and other internet-based psychological interventions are yet to be thoroughly examined, future research will probably reveal that such interventions can also be delivered effectively using digital health technologies. For example, similar to i-CBT, guided internet behavioural activation therapy is effective and superior to treatment as usual and psychoeducation in the treatment of less severe depression, and is no different to other behavioural therapies and mindfulness, and it can also be used adjunctively.
Psychological management strategy
A systematic approach should be adopted for psychological interventions. For less severe depression, specific psychological treatments can be prescribed as well as non-directive counselling and supportive therapy, and in many cases, offering psychological therapies in group settings might suffice. In contrast, in more severe depression, preference should be given to individual therapies of greater intensity that target the specific symptom profile of patients. In addition to recognised psychological interventions such as CBT and interpersonal therapy, non-specific, non-directive psychological strategies and supportive therapies such as counselling that alleviate stress will probably benefit patients who are reasonably well between episodes.
Antidepressants
Over 30 different antidepressants can be used to treat depression. They are usually prescribed by physicians, and their availability varies across different jurisdictions and health systems around the world. Having displaced tricyclics, which dominated during the 20th century, SSRIs are now the most widely prescribed antidepressants for the treatment of depression, and this shift towards newer medications has been accompanied by an increase in antidepressant prescriptions, which has made the management of depression more costly.
Antidepressant prescription requires careful deliberation of several factors, beginning with whether the patient wants to take medication and how well they cope with adverse effects should they occur, as tolerability affects medication adherence throughout management. Therefore, the administration of antidepressants, especially their commencement, should take place in an established therapeutic relationship and might require psychiatrist involvement. Importantly, transient adverse effects might occur upon initiation of antidepressant treatment, such as headache, nausea, or gastrointestinal issues, which typically cease within a week. However, if these symptoms persist, are severe, and/or are accompanied by other adverse effects, a treatment review is warranted to consider potentially withdrawing or switching the medication.
Antidepressant choice
Numerous factors can influence antidepressant prescribing choice, but the selection of an antidepressant should be based on patient characteristics, illness features, access to treatment, and its pharmacological properties, as well as medication history and whether any comorbidities are present. Patient characteristics such as age and gender are important due to interindividual biological variability in antidepressant distribution and metabolism, which play a crucial role in determining clinical response and the occurrence of adverse effects. Alongside these, it is also important to consider illness features that define the person’s depression such as symptom profile and illness severity. In practice, balancing the benefits of treatment against potential costs along with consideration of patient preferences usually helps decide which antidepressants are suitable. Another important consideration is the treatment setting (eg, hospitals, specialist outpatient centres, primary care, or within the community) as this affects the ability to monitor treatment. However, all these important considerations are only pertinent if a medication is available and can be readily accessed.
Beyond knowing whether a particular antidepressant is effective, its specific efficacy is not an important factor when deciding treatment choice. This is because, compared with placebo, most antidepressants are equally efficacious. The reason for this homogeneous effect is not fully known, but it might be a consequence of antidepressant mechanisms converging downstream, both intracellularly and functionally (eg, within neural networks). Furthermore, in real-world primary care settings, antidepressants only achieve small-to-medium effectiveness with moderate-to-high tolerability and low acceptability. Consequently, SSRIs are the most commonly prescribed first-line agents irrespective of severity and setting, whereas prescription patterns of other antidepressants vary. This is because SSRIs are generally better tolerated and safer than most other antidepressants, particularly older agents.
In recent clinical guidelines, recommendations about antidepressant choice are based on depression severity, rated broadly as less or more severe (as per the UK National Institute for Health and Care Excellence guidelines), or clinical factors such as efficacy and tolerability (eg, the Royal Australian and New Zealand College of Psychiatrists guidelines), and medication options are sequenced as first-line, second-line, and third-line (eg, the Canadian Network for Mood and Anxiety Treatments). However, grading severity is not necessarily or always informative, and clinical symptom profiling might not meaningfully inform treatment choice. Furthermore, many contemporaneously published guidelines for managing depression advocate different approaches and position different antidepressants as first-line therapy, which suggests that the evidence does not definitively support superiority of any one strategy over another, and that in clinical practice, perhaps considering elements from all three approaches (lifestyle, psychological, and pharmacological) is apt.
Acute treatment: initiating antidepressant therapy
The pharmacotherapy of depression comprises three phases (acute, continuation, and maintenance) that are separated by transitions (ie, remission and recovery). Therefore, continuation and maintenance refer to long-term treatment that includes antidepressant discontinuation.
When commencing antidepressants, they should be prescribed at a third to a half of the recommended therapeutic dose and then gradually increased over 1–2 weeks to minimise the likelihood of adverse effects. This is because if adverse effects occur, patients might stop taking their medication and typically antidepressants take several weeks to produce discernible clinical improvement. Therefore, when commencing antidepressants or altering dose, a frank discussion of likely outcomes and the risks involved is essential, and regular follow-up and monitoring should be instituted. Additionally, patients should be aware that more than one antidepressant might need to be tried to achieve a satisfactory and sustained response; there are many different antidepressants available, each with unique actions and tolerability profiles; and in most cases depression resolves with treatment. However, knowing which antidepressant will work is largely contingent on trialling the medication, because in community settings, prediction based on baseline characteristics alone has limited accuracy. Therefore, measurement-based care, including mood monitoring for example, and systematic outcome assessment are important, as early response to treatment remains a useful clinical indicator of eventual outcomes. Of those that respond poorly to an antidepressant, 35–67% of patients are likely to eventually improve if an alternative strategy is adopted, such as switching to another antidepressant, adding another medication, or adding or switching to a psychological intervention.
In the management of depression, the initial few weeks before and after starting any treatment is a high risk period for suicide, and although antidepressants generally reduce suicidal ideation, a small proportion of patients, especially young people, might experience increased suicidal ideation when initiating antidepressant therapy.
Continuation and maintenance phase: long-term treatment
The treatments prescribed for an acute episode of depression will probably be continued into maintenance therapy, and therefore many of the same considerations (eg, tolerability and antidepressant response that apply at the outset) remain relevant throughout the course of long-term treatment. To be confident of preventing relapse, continuation and maintenance treatment should jointly last for at least 6–9 months and ideally a year. Once a person has fully recovered, antidepressant treatment should be gradually withdrawn—slowly tapering medication dosage accompanied by structured psychological support. However, stopping antidepressant therapy is not straightforward and discontinuation of antidepressant treatment requires careful planning and close monitoring, especially since a third of patients who discontinue treatment will have discontinuation symptoms, and as many as one in 30 cases might be severe.
Non-response and treatment of depression in different populations
Management of depression in adolescents and older adults, as well as the needs of managing peripartum depression and depression occurring in the context of physical diseases, require additional considerations that are beyond the scope of this Seminar. In many of these contexts, outcomes are poor, which is a problem that affects depression more generally and is being researched within the concept of treatment-resistant depression. In each of these clinical situations, the diagnosis and management of depression must be tailored and is best informed by additional guidance that is specific to population needs.
In addition to the established treatments and mainstream management strategies discussed in this Seminar, there are many novel complementary and innovative interventions for the treatment of depression that are under investigation and initial findings appear promising, although evidence to date for these interventions is weak. However, a detailed discussion of these new and emerging therapies is beyond the scope of this Seminar, especially as many have limited availability. As patients might ask about these interventions, their potential uses are summarised in the appendix.
Conclusion
Depression is common throughout adulthood, and psychoeducation, lifestyle modifications, and psychological interventions might help anticipate acute exacerbations and limit illness duration. Treatments for depression are as multifaceted as the illness itself. A large proportion of patients will require multiple treatments to regain normal functioning, some will require referral to specialists and hospitalisation, and a few might never fully recover. Therefore, research into the development of new medications remains crucial alongside improving diagnosis and management using existing knowledge and treatments.
Panel 1 から Panel 9 まで
Panel 1: Depression vulnerability factors
Biological and physical health factors
Immutable factors
- Family history of mental illness*
- Mood disorder
- Substance misuse
- Epilepsy
- Intellectual disability
- Head injury
- Concussion
- Traumatic brain injury
Modifiable factors
- Physical condition
- Cardiovascular (eg, hypertension and cardiovascular disease)
- Neurological (eg, dementia and Parkinson’s disease)
- Metabolic (eg, diabetes and hypothyroidism)
- Lifestyle
- Unbalanced diet
- Lack of or irregular exercise
- Deprivation or non-restorative sleep
- Poor sleep hygiene
- Smoking and consumption of drugs and alcohol
Psychological and mental health factors
Immutable factors
- Personal history of mental illness
- Mood disorders (eg, depression and bipolar disorder)
- Substance misuse (eg, alcohol and cannabis)
Modifiable factors
- Mental condition
- Anxiety
- Psychosis
- Eating disorders
- Substance use
- Personality
- Insecure attachment
- Negative self-concept
- Sensitivity to rejection
- Negative emotionality
- Perfectionism
- Pessimism
- Low resilience
- Maladaptive coping strategies
- Rumination
Social and economic factors
Immutable factors
- Previous stressful life events
- Loss (eg, death of parents, siblings, or spouse; financial loss; or loss of identity)
- Past experience of abuse
- Childhood abuse (physical, emotional, or sexual)
- Partner or parental abuse (verbal, physical, sexual, or financial)
- Bullying at school by peers or teachers
- Harassment and bullying by co-workers and managers
Modifiable factors
- Current experience of abuse
- Parental or partner abuse (verbal, physical, sexual, or financial)
- Workplace harassment and bullying by co-workers, line managers, or organisation
- Lack of social support
- Social exclusion due to one’s values, belief, or identity
- Low socioeconomic status
- Unemployment
- Low income
- Unstable housing
- Threats to safety and security
- Unsafe living conditions
- Insecure housing
- Persecution and war
*Family history of mental illness reflects not only biological vulnerabilities via genetics, but also environmental risk factors associated with mental illness (eg, effects on parenting) as well as contextual risk factors (eg, poverty).
Panel 2: Watchful waiting in primary care
Diagnosing depression requires a person-centred approach. General practitioners (GPs) are suitable for this approach as they provide whole person care in the context of a doctor–patient relationship. Formulating depression requires skilful integration of biopsychosocial and biographical information and GPs are well positioned in this regard as the patient is usually well known to them. This familiarity also enables GPs to distinguish between situational crises and clinical depression and function as gatekeepers as they determine which pathway of care to pursue and when to refer to a specialist.
This process is sometimes called watchful waiting as it takes time and entails careful appraisal. During this time, which can vary considerably from days to weeks, collateral information can be sought, and investigations that help exclude medical causes of depression, such as anaemia and hypothyroidism, can be conducted; this approach is also helpful because it lends further credence to the patient’s distress. Hence, watchful waiting is in fact an active process that allows other sources of distress such as pain or infection to be treated, and its principal aim is to allow sufficient time to lapse so that a proper diagnosis of depression can be made and suitable management can be determined.
However, watchful waiting is not always appropriate, for example, in crisis situations such as severe depression or suicidal risk, in which practical steps might need to be taken immediately to treat the patient and ensure their safety. In these cases, mood monitoring should be instituted.
Panel 3: Mood monitoring
Once depression is being considered by a health-care professional, patients should record their clinical symptoms, sleep, and physical activity. Asking patients to monitor themselves helps them and the health-care professional to understand the nature of their symptoms and provides a longitudinal record that is less reliant solely on the patient’s long-term recall. Monitoring symptoms is also useful during management as it helps evaluate treatment outcomes.
Digital health technologies—any form of technology for health care, such as the use of smartphones to monitor health or provide guidance—could assist with mood monitoring. The term also refers to messaging, digital phenotyping, and the use of wearables such as activity trackers, as well as the use of telehealth and videoconferencing. Digital health technologies are used to provide psychoeducation, reminders, mood monitoring, and the delivery of psychological interventions.
Panel 4: Suicidal thoughts and risk of suicide
Suicidal thoughts often occur in the context of depression and can be confusing as they are a diagnostic feature of the illness but also a cause for concern. Thoughts about suicide are usually driven by critical thoughts about oneself, one’s relationships, and one’s situation in life. Negative thinking and feelings such as guilt can fuel a sense of helplessness and lead to a loss of hope, which can prompt thoughts about ending one’s life, especially to avoid continuing psychological pain.
Therefore, when assessing a patient with depression, it is important to enquire about thoughts of suicide or self-harm, and when formulating an individual’s risk of self-harm or suicide, examining their specific needs and how best to ensure their safety is crucial. Regarding suicidal thoughts, it is important to assess their nature (frequency, duration, and content), as well as the process of suicidal ideation (the individual’s conviction and intent and any plans they might have made). Ideally, a formulation of suicide risk should include consideration of historical factors (eg, previous suicide attempts), recent difficulties, and the availability of resources such as family support. If there is serious concern regarding a person’s safety or there is an ongoing risk of self-harm, a referral should be made to specialist or emergency services, and hospitalisation might be indicated.
Panel 5: Risky lifestyle habits
In most countries, it is legal to smoke tobacco and drink alcohol and therefore they are by far the most common risky lifestyle habits, and their use is well documented and researched.
Alcohol misuse
Links between alcohol misuse and depression are both direct and indirect as alcohol is a depressant, and once dependent, individuals continue to misuse alcohol to transiently alleviate stress. Managing depression in the context of alcohol misuse (dual diagnosis) is complicated and usually requires specialist services. Many specialist services treat the two disorders concurrently. However, in most cases, substance misuse must be tackled first before depression can be treated. This is because addressing alcohol consumption often reduces depressive symptoms, and implementing strategies to address problematic alcohol use early in the management of depression (eg, with psychological interventions) increases the chance of benefiting from depression treatments.
Smoking tobacco
Smoking is linked to heart disease, cancer, and metabolic disorders; there are no health benefits from this habit even though the inhalation of nicotine is initially anxiolytic. This anti-anxiety effect soon diminishes with repeated use and gives way to nicotine craving. Such gradual habituation and dependence are also evident in those who vape, and this is particularly concerning as this habit is increasingly common in adolescents and young adults. Contrary to the misconception that smoking cessation might increase anxiety and depression, those who stop smoking usually experience an improvement in ensuing months for these symptoms.
Panel 6: Sleep pharmacotherapy
Benzodiazepines and related medications can be effective sedatives if used in the short term (<4 weeks), but their use to modify sleep to treat depression is less well mapped and their prescription (both as monotherapy and adjunctive treatment to antidepressants) does not show sustained benefits. These medications should therefore be prescribed with caution and only for a limited time, after which they should be discontinued with gradual dose reduction.
Tricyclics have long been used to aid sleep and treat depression, and more recently, antipsychotics that are sedating (eg, quetiapine) have been prescribed for similar reasons as they help with initial insomnia and short-term relief of anxiety. However, the adverse effects of these medications limit their benefit in the long term. Other medications that are used for sleep (eg, melatonin and orexin) appear to be effective in instituting normal sleep cycles, but again, specific benefits in the context of depression have not yet been established. Notably, melatonin supplementation has only shown significant efficacy at higher doses and after 12 weeks of treatment, and orexin antagonists have not shown consistent effectiveness in the treatment of depression.
Panel 7: Risk of suicide and antidepressants
The risk of suicidality (suicidal thinking or behaviour) is increased in adolescents and young people. Therefore, in the USA, many agents carry a US Food & Drug Administration black-box warning. In the UK, the safety warning from the Medicine and Healthcare products Regulatory Agency states that suicidal acts and behaviour are increased with the use of selective serotonin reuptake inhibitors and serotonin–norepinephrine reuptake inhibitors in people younger than 25 years, and that the risks for specific antidepressants outweigh the benefits. Therefore, these antidepressants should not be used in this patient age group.
Consequently, routine monitoring of suicide is recommended in patients receiving antidepressant treatment, particularly at the outset (for the first 4 weeks or so) following the initiation of a new medication, and also after stopping treatment, and this message should also be included in any psychoeducation that is provided.
Panel 8: Antidepressant discontinuation syndrome
Symptoms
- Mainly mild, reversible, non-specific, and physical in nature
- Peak: 36–96 hours
- Rapid onset within 1 week of discontinuation (3–5 half-lives)
- Resolve: Spontaneously (usually within 2 weeks), but might take longer (up to 6 weeks) depending on half-life; or if medication is resumed
Risk for individual antidepressants
- Very high: phenelzine and tranylcypromine
- High: tricyclic antidepressants, venlafaxine, desvenlafaxine, and paroxetine
- Moderate: sertraline, citalopram, escitalopram, duloxetine, and vortioxetine
- Low: fluoxetine and milnacipran
- No risk: agomelatine
- Unclear or unknown: mirtazapine and bupropion
Panel 9: Complementary treatments and emerging therapies
Complementary treatments
Complementary treatments include herbal compounds and nutraceuticals. Inconsistency of therapeutic dose ranges for most complementary treatments and lack of sufficient evidence, which is on par with that for antidepressants and psychological interventions, means that they are only recommended for treating less severe depression, but can be used adjunctively for more severe depression.
Herbal compounds include St John’s Wort, saffron, lavender, and roseroot. Of these, only St John’s Wort has evidence of efficacy in less severe depression. Hence, they are positioned as third-line treatments in the Canadian Network for Mood and Anxiety Treatments’ guidelines. Similarly, nutraceuticals (unregulated substances derived from natural sources), including dietary supplements and food additives such as omega-3 fatty acids and dehydroepiandrosterone, are regarded as second-line or third-line treatments for depression.
Emerging therapies
In recent years, renewed interest in developing novel treatments for depression has been fuelled by increasing frustration with existing therapies. Almost a third of patients with depression have a poor response to at least two adequate courses of currently available antidepressants and are referred to as treatment-resistant. As most antidepressants act on monoaminergic pathways, alternative mechanisms of action have been sought, often with the additional aim of having more immediate impact.
- Ketamine and esketamine: Ketamine is an established dissociative anaesthetic that has been found to have psychoactive properties at subanaesthetic doses. Binding to glutamate receptors, ketamine and its s-enantiomer (esketamine) reduce the symptoms of depression and suicide thoughts. As such, intravenous ketamine is already used in the UK National Health Service to treat severe depression as an alternative to electroconvulsive therapy. However, even though the administration of intranasal esketamine and oral ketamine is easier, their use is limited partly due to limited long-term effects and the risk of dependence, but also due to the high cost of esketamine. Hence, the National Institute for Health and Care Excellence does not endorse its use, and the US Food & Drug Administration has only approved esketamine as an adjunctive therapy to be administered alongside an oral antidepressant. A similar combination of ketamine with psychotherapy for depression is also available in the USA and the UK but this is not evidence-based.
- Brexanolone: Brexanolone is a neurosteroid that structurally resembles endogenous allopregnanolone. It is a GABAergic system neuromodulator that enhances GABA signalling, a reduction in which has been found in women at risk for postpartum depression. Clinical trials have found it to be effective in this population and therefore it has an indication for postpartum depression. Zuranolone—an allosteric GABA receptor modulator—is also showing antidepressant potential in early clinical trials.
- Medicinal cannabis: Components of Cannabis sativa are thought to have therapeutic potential and, in jurisdictions where medicinal cannabis products are licensed, these are increasingly being self-administered to treat a range of medical and psychiatric conditions. Although the main use of medicinal cannabis is for chronic pain, anxiety, sleep disorders, and post-traumatic stress disorder, individuals with depression are also taking specific formulations. However, although there is some preliminary evidence regarding the use of medicinal cannabis in anxiety, the evidence for its use specifically in depression is scarce (ie, its use to treat depression is not evidence-based). This is probably because, of the several hundred compounds within cannabis, tetrahydrocannabinol and cannabidiol are the most common, and while tetrahydrocannabinol is psychoactive (ie, causes a high), cannabidiol is not. However, in practice and especially in jurisdictions where there is no regulation of medicinal cannabis-containing products, those that are labelled as cannabidiol might contain tetrahydrocannabinol and might not be accurately labelled. Hence there is potential for substantial misuse of medicinal cannabis.
- Psychedelics: Psychedelics have a long history of use in healing as well as in ceremonies of religious and spiritual importance. A resurgence of interest in the past two decades has brought several agents to the fore, many of which are administered alongside psychotherapeutic interventions.
- Psilocybin: found in specific species of fungi and is consumed orally in the treatment of depression alongside psychological support. Recent research suggests it might have some benefit in select cases, but emerging evidence also points to a potential increase in suicidality. Hence, it is only available under supervision in approved health-care settings.
- Ayahuasca: a traditional Amazonian plant medicine that is brewed to extract the hallucinogen dimethyltryptamine. Preliminary randomised controlled trials suggest a rapid but very short-lived antidepressant effect, with the majority of those injecting ayahuasca vomiting and many having severe nausea.
- Other molecules: currently being investigated for their use in psychiatric disorders include 3,4-methylenedioxymethamphetamine (MDMA; also known as ecstasy). Currently MDMA has only been licensed for use in the context of MDMA-assisted therapy for the treatment of post-traumatic stress disorder, and there is currently no evidence for its use in the treatment of depression.
- Anti-inflammatory medications and agents:
- Minocycline: an established tetracycline antibiotic that treats a broad spectrum of bacterial infections, including acne. It has been trialled in the treatment of depression (treatment-resistant and comorbid) both as monotherapy and adjunctive to antidepressants, and has been found to have variable benefit. It is well tolerated but further research to establish its therapeutic profile as an antidepressant is under way.
- Neuropeptide Y: produced in neurons and is involved in physiological regulatory processes including inflammatory mechanisms implicated in depression. When administered intranasally alongside an antidepressant, it appears to produce a rapid antidepressant effect that is short-lived. Although promising, as it builds on the inflammatory hypothesis of depression, further research is needed.
- Celecoxib: a non-steroidal anti-inflammatory drug used commonly for arthritic pain—has been found to have an antidepressant effect when prescribed adjunctively.
- Omega-3 fatty acids and cholesterol-lowering statins: have been found to be effective when administered alongside antidepressants in treating depression, and omega-3 fatty acids are also useful as monotherapy; however long-term benefits need further research.
- Probiotics: contain live microorganisms and have been investigated for antidepressant effects based on the hypothesis that gut alterations in microbiota can affect mental illnesses via gut–brain communication. Specific probiotic strains appear promising and might work by modifying the production of neurotransmitter precursors in the gut and countering inflammatory processes.
- Prebiotics: consist of non-digestible fibre that stimulate gut bacteria selectively and might also be of benefit in treating depression; however further research is needed.
- Microbiome-targeted therapies:
- Faecal microbiota transplantation: involves the transfer of faecal matter from a healthy person into the digestive system of a patient with depression. The aim is to restore the microbial composition of the gut. The process of faecal microbiota transplantation has shown encouraging results but further research is needed to understand the relationship between gut bacteria and depression and how altering the gut microbiota can alter mood.
1ページ目「Search strategy and selection criteria」
Search strategy and selection criteria
In this Seminar, to capture the many facets of depression, we drew on our unique expertise (psychiatry [GSM], primary health care [AS], nursing [C-YW], lived experience [AN], and psychology and neuroscience [VK and EB]) and clinical experience, and evidence from primary sources in relation to depression in adults was appraised collectively. Throughout this process, the Seminar was co-produced with an author with lived experience being involved from the outset. We drew upon recently published international guidelines and their analysis of evidence for the efficacy of various treatments, including those for the UK, Canada, the USA, and Australia and New Zealand, the Mental Health Gap Action Programme (mhGAP) Guideline for Mental and Neurological and Substance Use Disorders, and the World Federation of Societies of Biological Psychiatry. Some guidelines such as the mhGAP require minimal training, which is ideal for primary care.
Additionally, PubMed, APA PsycInfo, and Cochrane were searched using the search term “depressi*” or “mood disorder*” combined with other terms related to screening, diagnosis, formulation, and management. We restricted the search to papers from Jan 1, 2021, to Sept 1, 2025, with a focus largely on meta-analyses and systematic reviews and original research articles where relevant. The reference lists of included articles were scanned for relevant information and seminal articles outside this range have been included, where deemed helpful or necessary. A full list of search terms can be found in the appendix (p 18).
Separately, based on the data and in conjunction with clinical experience, we developed clinical advice for physicians and health workers in primary care and psychiatric services, specifically for general practitioners, psychiatrists, and psychologists. We have indicated areas in which evidence is absent or as yet insufficient. Clinical suggestions and recommendations have been made with treatment interventions in mind to inform therapeutic decision making and facilitate pathways of care (eg, treatment choices). Where possible, essential knowledge has been summarised and presented in figures to facilitate learning and understanding.
提供された文献の14ページから19ページに掲載されている「References」(参考文献リスト1〜228)を抽出し、改行や表記のブレなどを調整した上で、英文のまま出力します。
References
- WHO. Depressive disorder (depression). Aug 29, 2025. https://www.who.int/news-room/fact-sheets/detail/depression (accessed Feb 14, 2025).
- Institute of Health Metrics and Evaluation. GBD results. 2021. Global health data exchange. https://vizhub.healthdata.org/gbd-results/ (accessed June 1, 2024).
- Campbell D, Green MJ, Davies N, et al. Effects of depression on employment and social outcomes: a mendelian randomisation study. J Epidemiol Community Health 2022; 76: 563–71.
- Elmarasi M, Fuehrlein B. US Medicaid program: an analysis of the spending and utilization patterns for antidepressants from 2017 to 2021. Explor Res Clin Soc Pharm 2023; 13: 100392.
- McGrath JJ, Al-Hamzawi A, Alonso J, et al. Age of onset and cumulative risk of mental disorders: a cross-national analysis of population surveys from 29 countries. Lancet Psychiatry 2023; 10: 668–81.
- Obuobi-Donkor G, Nkire N, Agyapong VIO. Prevalence of major depressive disorder and correlates of thoughts of death, suicidal behaviour, and death by suicide in the geriatric population—a general review of literature. Behav Sci 2021; 11: 142.
- Rong J, Wang X, Cheng P, Li D, Zhao D. Global, regional and national burden of depressive disorders and attributable risk factors, from 1990 to 2021: results from the 2021 Global Burden of Disease study. Br J Psychiatry 2025; 227: 688–97.
- Marx W, Penninx BWJH, Solmi M, et al. Major depressive disorder. Nat Rev Dis Primers 2023; 9: 44.
- Platt JM, Bates L, Jager J, McLaughlin KA, Keyes KM. Is the US gender gap in depression changing over time? A meta-regression. Am J Epidemiol 2021; 190: 1190–206.
- Thapar A, Eyre O, Patel V, Brent D. Depression in young people. Lancet 2022; 400: 617–31.
- Kuehner C. Why is depression more common among women than among men? Lancet Psychiatry 2017; 4: 146–58.
- Solmi M, Radua J, Olivola M, et al. Age at onset of mental disorders worldwide: large-scale meta-analysis of 192 epidemiological studies. Mol Psychiatry 2022; 27: 281–95.
- Eaton WW, Shao H, Nestadt G, Lee HB, Bienvenu OJ, Zandi P. Population-based study of first onset and chronicity in major depressive disorder. Arch Gen Psychiatry 2008; 65: 513–20.
- Burcusa SL, Iacono WG. Risk for recurrence in depression. Clin Psychol Rev 2007; 27: 959–85.
- Verduijn J, Verhoeven JE, Milaneschi Y, et al. Reconsidering the prognosis of major depressive disorder across diagnostic boundaries: full recovery is the exception rather than the rule. BMC Med 2017; 15: 215.
- Ten Have M, Penninx BWJH, Tuithof M, et al. Duration of major and minor depressive episodes and associated risk indicators in a psychiatric epidemiological cohort study of the general population. Acta Psychiatr Scand 2017; 136: 300–12.
- Herrman H, Patel V, Kieling C, et al. Time for united action on depression: a Lancet–World Psychiatric Association Commission. Lancet 2022; 399: 957–1022.
- Schildkraut JJ. The catecholamine hypothesis of affective disorders: a review of supporting evidence. Am J Psychiatry 1965; 122: 509–22.
- Cui L, Li S, Wang S, et al. Major depressive disorder: hypothesis, mechanism, prevention and treatment. Signal Transduct Target Ther 2024; 9: 30.
- Goldstein-Piekarski AN, Ball TM, Samara Z, et al. Mapping neural circuit biotypes to symptoms and behavioral dimensions of depression and anxiety. Biol Psychiatry 2022; 91: 561–71.
- Long F, Chen Y, Zhang Q, et al. Predicting treatment outcomes in major depressive disorder using brain magnetic resonance imaging: a meta-analysis. Mol Psychiatry 2025; 30: 825–37.
- Ogunmoroti O, Osibogun O, Spatz ES, et al. A systematic review of the bidirectional relationship between depressive symptoms and cardiovascular health. Prev Med 2022; 154: 106891.
- Russell G, Lightman S. The human stress response. Nat Rev Endocrinol 2019; 15: 525–34.
- Clerici L, Bottari D, Bottari B. Gut microbiome, diet and depression: literature review of microbiological, nutritional and neuroscientific aspects. Curr Nutr Rep 2025; 14: 30.
- UK National Institute for Health and Care Excellence. Depression in adults: treatment and management. June 29, 2022. UK National Institute for Health and Care Excellence. https://www.nice.org.uk/guidance/ng222 (accessed June 1, 2024).
- Malhi GS, Mann JJ. Depression. Lancet 2018; 392: 2299–312.
- Vinkers CH, Kuzminskaite E, Lamers F, Giltay EJ, Penninx BWJH. An integrated approach to understand biological stress system dysregulation across depressive and anxiety disorders. J Affect Disord 2021; 283: 139–46.
- Sălcudean A, Popovici R-A, Pitic DE, et al. Unraveling the complex interplay between neuroinflammation and depression: a comprehensive review. Int J Mol Sci 2025; 26: 1645.
- Yuan M, Yang B, Rothschild G, et al. Epigenetic regulation in major depression and other stress-related disorders: molecular mechanisms, clinical relevance and therapeutic potential. Signal Transduct Target Ther 2023; 8: 309.
- Kendall KM, Van Assche E, Andlauer TFM, et al. The genetic basis of major depression. Psychol Med 2021; 51: 2217–30.
- Remes O, Mendes JF, Templeton P. Biological, psychological, and social determinants of depression: a review of recent literature. Brain Sci 2021; 11: 1633.
- Wimbarti S, Kairupan BHR, Tallei TE. Critical review of self-diagnosis of mental health conditions using artificial intelligence. Int J Ment Health Nurs 2024; 33: 344–58.
- Capurro D, Coghlan S, Pires DEV. Preventing digital overdiagnosis. JAMA 2022; 327: 525–26.
- Hochberg I, Allon R, Yom-Tov E. Assessment of the frequency of online searches for symptoms before diagnosis: analysis of archival data. J Med Internet Res 2020; 22: e15065.
- Demyttenaere K. The temporal experience in depression: from slowing down and delayed help seeking to the emergency setting and length of treatment. Int Rev Psychiatry 2022; 34: 693–98.
- McLaren T, Peter L-J, Tomczyk S, Muehlan H, Schomerus G, Schmidt S. The Seeking Mental Health Care model: prediction of help-seeking for depressive symptoms by stigma and mental illness representations. BMC Public Health 2023; 23: 69.
- Pescosolido BA, Halpern-Manners A, Luo L, Perry B. Trends in public stigma of mental illness in the US, 1996–2018. JAMA Network Open 2021; 4: e2140202.
- Mekonen T, Chan GCK, Connor JP, Hides L, Leung J. Estimating the global treatment rates for depression: a systematic review and meta-analysis. J Affect Disord 2021; 295: 1234–42.
- Thombs BD, Markham S, Rice DB, Ziegelstein RC. Does depression screening in primary care improve mental health outcomes? BMJ 2021; 374: n1661.
- WHO. International statistical classification of diseases and related health problems (11th revision). January, 2022. World Health Organization. https://www.who.int/standards/classifications/classification-of-diseases (accessed May 1, 2024).
- American Psychiatric Association. Diagnostic and statistical manual of mental disorders: DSM-5-TR, 5th edn. Washington, DC: American Psychiatric Association, 2022.
- Lam RW, Kennedy SH, Adams C, et al. Canadian Network for Mood and Anxiety Treatments (CANMAT) 2023 update on clinical guidelines for management of major depressive disorder in adults: Réseau Canadien pour les Traitements de l’Humeur et de l’Anxiété (CANMAT) 2023: mise à jour des lignes directrices cliniques pour la prise en charge du trouble dépressif majeur chez les adultes. Can J Psychiatry 2024; 69: 641–87.
- American Psychological Association. Clinical practice guideline for the treatment of depression across three age cohorts. June, 2025. https://www.apa.org/depression-guideline (accessed Aug 1, 2025).
- Malhi GS, Bell E, Bassett D, et al. The 2020 Royal Australian and New Zealand College of Psychiatrists clinical practice guidelines for mood disorders. Aust N Z J Psychiatry 2021; 55: 7–117.
- De Maeseneer J, Li D, Palsdottir B, et al. Universal health coverage and primary health care: the 30 by 2030 campaign. Bull World Health Organ 2020; 98: 812–14.
- Innocenti F, McCormick B, Nicodemo C. Gatekeeping in primary care: analysing GP referral patterns and specialist consultations in the NHS. Econ Model 2025; 142: 106925.
- Kostic M, Milojevic T, Buzejic J, et al. Watchful waiting for depression using depathologization, advice and shared decision making. J Affect Disord Rep 2024; 16: 100753.
- Trimmel K, Eder HG, Böck M, Stefanic-Kejik A, Klösch G, Seidel S. The (mis)perception of sleep: factors influencing the discrepancy between self-reported and objective sleep parameters. J Clin Sleep Med 2021; 17: 917–24.
- Baryshnikov I, Aledavood T, Rosenström T, et al. Relationship between daily rated depression symptom severity and the retrospective self-report on PHQ-9: a prospective ecological momentary assessment study on 80 psychiatric outpatients. J Affect Disord 2023; 324: 170–74.
- Naik N, Hameed BMZ, Sooriyaperakasam N, et al. Transforming healthcare through a digital revolution: a review of digital healthcare technologies and solutions. Front Digit Health 2022; 4: 919985.
- Torous J, Bucci S, Bell IH, et al. The growing field of digital psychiatry: current evidence and the future of apps, social media, chatbots, and virtual reality. World Psychiatry 2021; 20: 318–35.
- Philippe TJ, Sikder N, Jackson A, et al. Digital health interventions for delivery of mental health care: systematic and comprehensive meta-review. JMIR Ment Health 2022; 9: e35159.
- Nock MK, Jaroszewski AC, Deming CA, et al. Antecedents, reasons for, and consequences of suicide attempts: results from a qualitative study of 89 suicide attempts among army soldiers. J Psychopathol Clin Sci 2025; 134: 6–17.
- UK National Institute for Health and Care Excellence. Self-harm: assessment, management and preventing recurrence. Sept 7, 2022. https://www.nice.org.uk/guidance/ng225/resources/selfharm-assessment-management-and-preventing-recurrence-pdf-66143837346757 (accessed May 1, 2024).
- Simon GE, Moise N, Mohr DC. Management of depression in adults: a review. JAMA 2024; 332: 141–52.
- Malhi GS, Bell E, Bassett D, et al. Difficult decision-making in major depressive disorder: practical guidance based on clinical research and experience. Bipolar Disord 2023; 25: 355–78.
- Moriarty AS, Meader N, Snell KIE, et al. Predicting relapse or recurrence of depression: systematic review of prognostic models. Br J Psychiatry 2022; 221: 448–58.
- Fritz K, Russell AMT, Allwang C, Kuiper S, Lampe L, Malhi GS. Is a delay in the diagnosis of bipolar disorder inevitable? Bipolar Disord 2017; 19: 396–400.
- Tyrer P, Yang M, Tyrer H, Malhi G. Factors predisposing to the onset of bipolar disorder: a 30-year longitudinal study. Bipolar Disord 2025; 27: 310–15.
- Simonsmeier BA, Flaig M, Simacek T, Schneider M. What sixty years of research says about the effectiveness of patient education on health: a second order meta-analysis. Health Psychol Rev 2022; 16: 450–74.
- Kürümlüoğlugil R, Tanrıverdi D. The effects of the psychoeducation on cognitive distortions, negative automatic thoughts and dysfunctional attitudes of patients diagnosed with depression. Psychol Health Med 2022; 27: 2085–95.
- Dell’Osso B, Albert U, Carrà G, et al. How to improve adherence to antidepressant treatments in patients with major depression: a psychoeducational consensus checklist. Ann Gen Psychiatry 2020; 19: 61.
- Rigabert A, Motrico E, Moreno-Peral P, et al. Effectiveness of online psychological and psychoeducational interventions to prevent depression: a systematic review and meta-analysis of randomized controlled trials. Clin Psychol Rev 2020; 82: 101931.
- Kivlichan AE, Praecht A, Wang C, George TP. Substance-induced mood disorders: a scoping review. Curr Addict Rep 2024; 11: 1–18.
- Charlet K, Heinz A. Harm reduction-a systematic review on effects of alcohol reduction on physical and mental symptoms. Addict Biol 2017; 22: 1119–59.
- Patel V, Saxena S, Lund C, et al. The Lancet Commission on global mental health and sustainable development. Lancet 2018; 392: 1553–98.
- Visontay R, Mewton L, Slade T, Aris IM, Sunderland M. Moderate alcohol consumption and depression: a marginal structural model approach promoting causal inference. Am J Psychiatry 2023; 180: 209–17.
- Firth J, Siddiqi N, Koyanagi A, et al. The Lancet Psychiatry Commission: a blueprint for protecting physical health in people with mental illness. Lancet Psychiatry 2019; 6: 675–712.
- Fredman Stein K, Allen JL, Robinson R, Smith C, Sawyer K, Taylor G. Do interventions principally targeting excessive alcohol use in young people improve depression symptoms?: a systematic review and meta-analysis. BMC Psychiatry 2022; 22: 417.
- Luoto KE, Lassila A, Leinonen E, Kampman O. Predictors of short-term response and the role of heavy alcohol use in treatment of depression. BMC Psychiatry 2023; 23: 880.
- Australian Institute of Health and Welfare. Young people’s use of vapes and e-cigarettes. Feb 29, 2024. Australian Government. https://www.aihw.gov.au/reports/smoking/young-peoples-vapes-e-cigarettes (accessed June 1, 2024).
- Wu AD, Gao M, Aveyard P, Taylor G. Smoking cessation and changes in anxiety and depression in adults with and without psychiatric disorders. JAMA Netw Open 2023; 6: e2316111.
- Li J, Wang H, Li M, et al. Effect of alcohol use disorders and alcohol intake on the risk of subsequent depressive symptoms: a systematic review and meta-analysis of cohort studies. Addiction 2020; 115: 1224–43.
- Weinberger AH, Kashan RS, Shpigel DM, et al. Depression and cigarette smoking behavior: a critical review of population-based studies. Am J Drug Alcohol Abuse 2017; 43: 416–31.
- Sato A, Eguchi E, Hayashi F, et al. A prospective study of the association between lifestyle and the risk of depressive symptoms. J Affect Disord 2025; 376: 269–79.
- Maurus I, Wagner S, Spaeth J, et al. EPA guidance on lifestyle interventions for adults with severe mental illness: a meta-review of the evidence. Eur Psychiatry 2024; 67: e80.
- Tang L, Zhang L, Liu Y, et al. Optimal dose and type of exercise to improve depressive symptoms in older adults: a systematic review and network meta-analysis. BMC Geriatr 2024; 24: 505.
- Noetel M, Sanders T, Gallardo-Gómez D, et al. Effect of exercise for depression: systematic review and network meta-analysis of randomised controlled trials. BMJ 2024; 384: e075847.
- Patel RA, Panche AN, Harke SN. Gut microbiome-gut brain axis depression: interconnection. World J Biol Psychiatry 2025; 26: 1–36.
- Tan C, Yan Q, Ma Y, Fang J, Yang Y. Recognizing the role of the vagus nerve in depression from microbiota-gut brain axis. Front Neurol 2022; 13: 1015175.
- Lu S, Zhao Q, Guan Y, et al. The communication mechanism of the gut–brain axis and its effect on central nervous system diseases: a systematic review. Biomed Pharmacother 2024; 178: 117207.
- Suda K, Matsuda K. How microbes affect depression: underlying mechanisms via the gut–brain axis and the modulating role of probiotics. Int J Molec Sci 2022; 23: 1172.
- Morais LH, Schreiber HL 4th, Mazmanian SK. The gut microbiota–brain axis in behaviour and brain disorders. Nat Rev Microbiol 2021; 19: 241–55.
- Hossain MN, Lee J, Choi H, Kwak Y-S, Kim J. The impact of exercise on depression: how moving makes your brain and body feel better. Phys Act Nutr 2024; 28: 43–51.
- Ross RE, VanDerwerker CJ, Saladin ME, Gregory CM. The role of exercise in the treatment of depression: biological underpinnings and clinical outcomes. Mol Psychiatry 2023; 28: 298–328.
- Staudacher HM, Teasdale S, Cowan C, Opie R, Jacka FN, Rocks T. Diet interventions for depression: review and recommendations for practice. Aust N Z J Psychiatry 2025; 59: 115–27.
- Wang B, Fan Y, Wang X, et al. Influence of lifestyle patterns on depression among adults with diabetes: a mediation effect of dietary inflammatory index. BMC Public Health 2024; 24: 1779.
- Mrozek W, Socha J, Sidorowicz K, et al. Pathogenesis and treatment of depression: role of diet in prevention and therapy. Nutrition 2023; 115: 112143.
- Marx W, Lane M, Hockey M, et al. Diet and depression: exploring the biological mechanisms of action. Mol Psychiatry 2021; 26: 134–50.
- Marx W, Lane MM, Hockey M, et al. Diet and depression: future needs to unlock the potential. Mol Psychiatry 2022; 27: 778–80.
- Koelman L, Egea Rodrigues C, Aleksandrova K. Effects of dietary patterns on biomarkers of inflammation and immune responses: a systematic review and meta-analysis of randomized controlled trials. Adv Nutr 2022; 13: 101–15.
- Yao H, Zhang D, Yu H, et al. The microbiota–gut-brain axis in pathogenesis of depression: a narrative review. Physiol Behav 2023; 260: 114056.
- Berg G, Rybakova D, Fischer D, et al. Microbiome definition re-visited: old concepts and new challenges. Microbiome 2020; 8: 103.
- Nicolaou M, Colpo M, Vermeulen E, et al. Association of a priori dietary patterns with depressive symptoms: a harmonised meta-analysis of observational studies. Psychol Med 2020; 50: 1872–83.
- Lassale C, Batty GD, Baghdadli A, et al. Healthy dietary indices and risk of depressive outcomes: a systematic review and meta-analysis of observational studies. Mol Psychiatry 2019; 24: 965–86.
- Gianfredi V, Dinu M, Nucci D, et al. Association between dietary patterns and depression: an umbrella review of meta-analyses of observational studies and intervention trials. Nutr Rev 2023; 81: 346–59.
- Chen GQ, Peng CL, Lian Y, Wang BW, Chen PY, Wang GP. Association between dietary inflammatory index and mental health: a systematic review and dose-response meta-analysis. Front Nutr 2021; 8: 662357.
- Molendijk M, Molero P, Ortuño Sánchez-Pedreño F, Van der Does W, Angel Martínez-González M. Diet quality and depression risk: a systematic review and dose-response meta-analysis of prospective studies. J Affect Disord 2018; 226: 346–54.
- Lin F, Chen X, Cai Y, et al. Accelerated biological aging as potential mediator mediates the relationship between pro-inflammatory diets and the risk of depression and anxiety: a prospective analysis from the UK biobank. J Affect Disord 2024; 355: 1–11.
- Gee B, Orchard F, Clarke E, Joy A, Clarke T, Reynolds S. The effect of non-pharmacological sleep interventions on depression symptoms: a meta-analysis of randomised controlled trials. Sleep Med Rev 2019; 43: 118–28.
- Brupbacher G, Gerger H, Zander-Schellenberg T, et al. The effects of exercise on sleep in unipolar depression: a systematic review and network meta-analysis. Sleep Med Rev 2021; 59: 101452.
- Baranwal N, Yu PK, Siegel NS. Sleep physiology, pathophysiology, and sleep hygiene. Prog Cardiovasc Dis 2023; 77: 59–69.
- Sun A, Wu X. Efficacy of non-pharmacological interventions on improving sleep quality in depressed patients: a systematic review and network meta-analysis. J Psychosom Res 2023; 172: 111435.
- Simon L, Steinmetz L, Feige B, Benz F, Spiegelhalder K, Baumeister H. Comparative efficacy of onsite, digital, and other settings for cognitive behavioral therapy for insomnia: a systematic review and network meta-analysis. Sci Rep 2023; 13: 1929.
- Tao L, Jiang R, Zhang K, et al. Light therapy in non-seasonal depression: an update meta-analysis. Psychiatry Res 2020; 291: 113247.
- Huang X, Tao Q, Ren C. A comprehensive overview of the neural mechanisms of light therapy. Neurosci Bull 2024; 40: 350–62.
- Fregna L, Attanasio F, Colombo C. Evaluating the impact of adjunct bright light therapy on subjective sleep quality in major depressive disorder. J Affect Disord 2024; 348: 175–78.
- Geoffroy PA, Schroder CM, Reynaud E, Bourgin P. Efficacy of light therapy versus antidepressant drugs, and of the combination versus monotherapy, in major depressive episodes: a systematic review and meta-analysis. Sleep Med Rev 2019; 48: 101213.
- Brandt J, Bressi J, Lê M-L, et al. Prescribing and deprescribing guidance for benzodiazepine and benzodiazepine receptor agonist use in adults with depression, anxiety, and insomnia: an international scoping review. EClinicalMedicine 2024; 70: 102507.
- Hutka P, Krivosova M, Muchova Z, et al. Association of sleep architecture and physiology with depressive disorder and antidepressants treatment. Int J Mol Sci 2021; 22: 1333.
- Lin C-Y, Chiang C-H, Tseng MM, Tam K-W, Loh E-W. Effects of quetiapine on sleep: a systematic review and meta-analysis of clinical trials. Eur Neuropsychopharmacol 2023; 67: 22–36.
- Mulder R, Hamilton A, Irwin L, et al. Treating depression with adjunctive antipsychotics. Bipolar Disord 2018; 20 (suppl 2): 17–24.
- Fagan H, Jones E, Baldwin DS. Orexin receptor antagonists in the treatment of depression: a leading article summarising pre-clinical and clinical studies. CNS Drugs 2023; 37: 1–12.
- Li C, Ma D, Li M, et al. The therapeutic effect of exogenous melatonin on depressive symptoms: a systematic review and meta-analysis. Front Psychiatry 2022; 13: 737972.
- Uğurlu M. Orexin receptor antagonists as adjunct drugs for the treatment of depression: a mini meta-analysis. Noro Psikiyatri Ars 2023; 61: 77–84.
- Krystal A, Blier P, Culpepper L, et al. Efficacy and safety of lemborexant in subjects with insomnia disorder receiving medications for depression or anxiety symptoms. Neuropsychopharmacol Rep 2025; 45: e12509.
- Eigenhuis E, van Buuren VEM, Boeschoten RE, Muntingh ADT, Batelaan NM, van Oppen P. The effects of patient preference on clinical outcome, satisfaction and adherence within the treatment of anxiety and depression: a meta-analysis. Clin Psychol Psychother 2024; 31: e2985.
- Voderholzer U, Barton BB, Favreau M, et al. Enduring effects of psychotherapy, antidepressants and their combination for depression: a systematic review and meta-analysis. Front Psychiatry 2024; 15: 1415905.
- dosReis S, Espinal Pena D, Fincannon A, Gorman EF, Amill-Rosario A. Discrete choice experiments to elicit patient preferences for the treatment of major depressive disorder: a systematic review. Patient 2025; 18: 19–33.
- Boschloo L, Bekhuis E, Weitz ES, et al. The symptom-specific efficacy of antidepressant medication vs cognitive behavioral therapy in the treatment of depression: results from an individual patient data meta-analysis. World Psychiatry 2019; 18: 183–91.
- Cohen ZD, DeRubeis RJ. Treatment selection in depression. Annu Rev Clin Psychol 2018; 14: 209–36.
- Schefft C, Heinitz C, Guhn A, Brakemeier E-L, Sterzer P, Köhler S. Efficacy and acceptability of third-wave psychotherapies in the treatment of depression: a network meta-analysis of controlled trials. Front Psychiatry 2023; 14: 1189970.
- Cuijpers P, Harrer M, Miguel C, Ciharova M, Karyotaki E. Five decades of research on psychological treatments of depression: a historical and meta-analytic overview. Am Psychol 2025; 80: 297–310.
- Cuijpers P, Quero S, Noma H, et al. Psychotherapies for depression: a network meta-analysis covering efficacy, acceptability and long-term outcomes of all main treatment types. World Psychiatry 2021; 20: 283–93.
- Cuijpers P, Miguel C, Harrer M, et al. Psychological treatment of depression: a systematic overview of a ‘meta-analytic research domain’. J Affect Disord 2023; 335: 141–51.
- Eubanks CF, Babl A. Are common factors responsible for therapeutic change? In: Leong FTL, Callahan JL, Zimmerman J, Constantino MJ, Eubanks CF, eds. APA handbook of psychotherapy: evidence-based practice, practice-based evidence, and contextual participant-driven practice, vol 2. American Psychological Association, 2024: 43–61.
- Bruijniks SJE, Meeter M, Lemmens LHJM, Peeters F, Cuijpers P, Huibers MJH. Temporal and specific pathways of change in cognitive behavioral therapy (CBT) and interpersonal psychotherapy (IPT) for depression. Behav Res Ther 2022; 151: 104010.
- A-Tjak JGL, Morina N, Topper M, Emmelkamp PMG. One year follow-up and mediation in cognitive behavioral therapy and acceptance and commitment therapy for adult depression. BMC Psychiatry 2021; 21: 41.
- Barsaglini A, Sartori G, Benetti S, Pettersson-Yeo W, Mechelli A. The effects of psychotherapy on brain function: a systematic and critical review. Prog Neurobiol 2014; 114: 1–14.
- Zhou Y, Zhao D, Zhu X, et al. Psychological interventions for the prevention of depression relapse: systematic review and network meta-analysis. Transl Psychiatry 2023; 13: 300.
- Buntrock C, Harrer M, Sprenger AA, et al, and the IPD-PrevDep Consortium. Psychological interventions to prevent the onset of major depression in adults: a systematic review and individual participant data meta-analysis. Lancet Psychiatry 2024; 11: 990–1001.
- Cuijpers P, Pineda BS, Quero S, et al. Psychological interventions to prevent the onset of depressive disorders: a meta-analysis of randomized controlled trials. Clin Psychol Rev 2021; 83: 101955.
- Gülpen J, Breedvelt JJF, van Dis EAM, et al. Psychological interventions for preventing relapse in individuals with partial remission of depression: a systematic review and individual participant data meta-analysis. Psychol Med 2025; 55: e50.
- Cuijpers P, Karyotaki E, Ciharova M, Miguel C, Noma H, Furukawa TA. The effects of psychotherapies for depression on response, remission, reliable change, and deterioration: a meta-analysis. Acta Psychiatr Scand 2021; 144: 288–99.
- Kopf-Beck J, Müller CL, Tamm J, et al. Effectiveness of schema therapy versus cognitive behavioral therapy versus supportive therapy for depression in inpatient and day clinic settings: a randomized clinical trial. Psychother Psychosom 2024; 93: 24–35.
- Cuijpers P, Miguel C, Harrer M, et al. Cognitive behavior therapy vs control conditions, other psychotherapies, pharmacotherapies and combined treatment for depression: a comprehensive meta-analysis including 409 trials with 52,702 patients. World Psychiatry 2023; 22: 105–16.
- Taylor CB, Graham AK, Flatt RE, Waldherr K, Fitzsimmons-Craft EE. Current state of scientific evidence on internet-based interventions for the treatment of depression, anxiety, eating disorders and substance abuse: an overview of systematic reviews and meta-analyses. Eur J Public Health 2021; 31 (suppl 1): i3–10.
- Wright JH, Owen JJ, Richards D, et al. Computer-assisted cognitive behavior therapy for depression: a systematic review and meta-analysis. J Clin Psychiatry 2019; 80: 3573.
- Andersson G, Carlbring P, Titov N, Lindefors N. Internet interventions for adults with anxiety and mood disorders: a narrative umbrella review of recent meta-analyses. Can J Psychiatry 2019; 64: 465–70.
- Zainal NH, Soh CP, Van Doren N, Benjet C. Do the effects of internet-delivered cognitive-behavioral therapy (i-CBT) last after a year and beyond? A meta-analysis of 154 randomized controlled trials (RCTs). Clin Psychol Rev 2024; 114: 102518.
- Karyotaki E, Efthimiou O, Miguel C, et al. Internet-based cognitive behavioral therapy for depression: a systematic review and individual patient data network meta-analysis. JAMA Psychiatry 2021; 78: 361–71.
- Palacios JE, Enrique A, Mooney O, et al. Durability of treatment effects following internet-delivered cognitive behavioural therapy for depression and anxiety delivered within a routine care setting. Clin Psychol Psychother 2022; 29: 1768–77.
- Krämer LV, Grünzig S-D, Baumeister H, Ebert DD, Bengel J. Effectiveness of a guided web-based intervention to reduce depressive symptoms before outpatient psychotherapy: a pragmatic randomized controlled trial. Psychother Psychosom 2021; 90: 233–42.
- Chen GJ, Kunik ME, Marti CN, Choi NG. Cost-effectiveness of tele-delivered behavioral activation by lay counselors for homebound older adults with depression. BMC Psychiatry 2022; 22: 648.
- Miguel C, Cristea IA, Karyotaki E. From clinical trials to real-world effectiveness: evaluating guided iCBT for depression in routine care. Lancet Psychiatry 2025; 12: 163–65.
- Duffy D, Richards D, Hisler G, Timulak L. Implementing internet-delivered cognitive behavioral therapy for depression and anxiety in adults: systematic review. J Med Internet Res 2025; 27: e47927.
- Linardon J, Messer M, Goldberg SB, Fuller-Tyszkiewicz M. The efficacy of mindfulness apps on symptoms of depression and anxiety: an updated meta-analysis of randomized controlled trials. Clin Psychol Rev 2024; 107: 102370.
- Huguet A, Miller A, Kisely S, Rao S, Saadat N, McGrath PJ. A systematic review and meta-analysis on the efficacy of internet-delivered behavioral activation. J Affect Disord 2018; 235: 27–38.
- UK National Institute for Health and Care Excellence. 1.5 Treatment for a new episode of less severe depression. June 29, 2022. UK National Institute for Health and Care Excellence. https://www.nice.org.uk/guidance/ng222/chapter/Recommendations#treatment-for-a-new-episode-of-less-severe-depression (accessed May 1, 2024).
- WHO. Group interpersonal therapy (IPT) for depression. Oct 3, 2016. World Health Organization. https://www.who.int/publications/i/item/WHO-MSD-MER-16.4 (accessed June 1, 2024).
- WHO. Mental Health Gap Action Programme (mhGAP) guideline for mental, neurological and substance use disorders. Nov 20, 2023. https://www.who.int/publications/i/item/9789240084278 (accessed June 1, 2024).
- UK National Institute for Health and Care Excellence. 1.6 Treatment for a new episode of more severe depression. June 29, 2022. UK National Institute for Health and Care Excellence. https://www.nice.org.uk/guidance/ng222/chapter/Recommendations#treatment-for-a-new-episode-of-more-severe-depression (accessed May 1, 2024).
- Hamdani SU, Zill-E-Huma, Zafar SW, et al. Effectiveness of relaxation techniques ‘as an active ingredient of psychological interventions’ to reduce distress, anxiety and depression in adolescents: a systematic review and meta-analysis. Int J Ment Health Syst 2022; 16: 31.
- Pereira VS, Hiroaki-Sato VA. A brief history of antidepressant drug development: from tricyclics to beyond ketamine. Acta Neuropsychiatr 2018; 30: 307–22.
- Jorgensen A, Larsen EN, Sloth MMB, Kessing LV, Osler M. Prescription patterns in unipolar depression: a nationwide Danish register-based study of 113,175 individuals followed for 10 years. Acta Psychiatr Scand 2024; 149: 88–97.
- Malhi GS, Acar M, Kouhkamari MH, et al. Antidepressant prescribing patterns in Australia. BJPsych Open 2022; 8: e120.
- Karami H, Mehrizi R, Effatpanah M, et al. Uncovering antidepressant prescription patterns: a three-year analysis of outpatient trends. BMC Psychiatry 2025; 25: 90.
- Cipriani A, Furukawa TA, Salanti G, et al. Comparative efficacy and acceptability of 12 new-generation antidepressants: a multiple-treatments meta-analysis. Lancet 2009; 373: 746–58.
- Peano A, Calabrese F, Pechlivanidis K, et al. International trends in antidepressant consumption: a 10-year comparative analysis (2010–2020). Psychiatr Q 2025; 96: 241–55.
- Solmi M, Miola A, Croatto G, et al. How can we improve antidepressant adherence in the management of depression? A targeted review and 10 clinical recommendations. Br J Psychiatry 2021; 43: 189–202.
- Golder S, Medaglio D, O’Connor K, Hennessy S, Gross R, Gonzalez Hernandez G. Reasons for discontinuation or change of selective serotonin reuptake inhibitors in online drug reviews. JAMA Netw Open 2023; 6: e2323746.
- Kalfas M, Tsapekos D, Butler M, et al. Incidence and nature of antidepressant discontinuation symptoms: a systematic review and meta-analysis. JAMA Psychiatry 2025; 82: 896–904.
- Henssler J, Heinz A, Brandt L, Bschor T. Antidepressant withdrawal and rebound phenomena. Dtsch Arztebl Int 2019; 116: 355–61.
- Berber MJ. FINISH: remembering the discontinuation syndrome. Flu-like symptoms, insomnia, nausea, imbalance, sensory disturbances, and hyperarousal (anxiety/agitation). J Clin Psychiatry 1998; 59: 255.
- Ji M, Feng J, Liu G. Efficacy and safety of aripiprazole or bupropion augmentation and switching in patients with treatment-resistant depression or major depressive disorder: a systematic review and meta-analysis of randomized controlled trials. PLoS One 2024; 19: e0299020.
- Lenze EJ, Mulsant BH, Blumberger DM, et al. Efficacy, safety, and tolerability of augmentation pharmacotherapy with aripiprazole for treatment-resistant depression in late life: a randomised, double-blind, placebo-controlled trial. Lancet 2015; 386: 2404–12.
- Lundberg J, Cars T, Lööv S-Å, et al. Association of treatment-resistant depression with patient outcomes and health care resource utilization in a population-wide study. JAMA Psychiatry 2023; 80: 167–75.
- Boyce P, Hopwood M, Morris G, et al. Switching antidepressants in the treatment of major depressive disorder: when, how and what to switch to? J Affect Disord 2020; 261: 160–63.
- Rush AJ, Trivedi MH, Wisniewski SR, et al. Acute and longer-term outcomes in depressed outpatients requiring one or several treatment steps: a STAR*D report. *Am J Psychiatry* 2006; 163: 1905–17.
- Pigott HE, Kim T, Xu C, Kirsch I, Amsterdam J. What are the treatment remission, response and extent of improvement rates after up to four trials of antidepressant therapies in real-world depressed patients? A reanalysis of the STAR*D study’s patient-level data with fidelity to the original research protocol. *BMJ Open* 2023; 13: e063095.
- Min H, Alemi F. Insights into prescribing patterns for antidepressants: an evidence-based analysis. BMC Med Inform Decis Mak 2025; 25: 42.
- Kamp M, Lo CWH, Kokkinidis G, et al. Sociodemographic, clinical, and genetic factors associated with self-reported antidepressant response outcomes in the UK Biobank. Psychol Med 2025; 55: e80.
- Squassina A, Paribello P, Pinna M, et al. A naturalistic retrospective evaluation of the utility of pharmacogenetic testing based on CYP2D6 e CYP2C19 profiling in antidepressants treatment in a cohort of patients with major depressive disorder. Prog Neuropsychopharmacol Biol Psychiatry 2025; 137: 111292.
- Selph SS, McDonagh MS. Depression in children and adolescents: evaluation and treatment. Am Fam Physician 2019; 100: 609–17.
- Hetrick SE, McKenzie JE, Bailey AP, et al. New generation antidepressants for depression in children and adolescents: a network meta-analysis. Cochrane Database Syst Rev 2021; 5: CD013674.
- Fagiolini A, González Pinto A, Miskowiak KW, Morgado P, Young AH, Vieta E. Trazodone in the management of major depression among elderly patients with dementia: a narrative review and clinical insights. Neuropsychiatr Dis Treat 2023; 19: 2817–31.
- Payne JL, Meltzer-Brody S. Antidepressant use during pregnancy: current controversies and treatment strategies. Clin Obstet Gynecol 2009; 52: 469–82.
- Uguz F, Sahingoz M, Kose SA, et al. Antidepressants and menstruation disorders in women: a cross-sectional study in three centers. Gen Hosp Psychiatry 2012; 34: 529–33.
- Hilas O, Avena-Woods C. Potential role of mirtazapine in underweight older adults. Consult Pharm 2014; 29: 124–30.
- Maslej MM, Furukawa TA, Cipriani A, et al. Individual differences in response to antidepressants: a meta-analysis of placebo-controlled randomized clinical trials. JAMA Psychiatry 2021; 78: 490–97.
- De Crescenzo F, De Giorgi R, Garriga C, et al. Real-world effects of antidepressants for depressive disorder in primary care: population-based cohort study. Br J Psychiatry 2024; 226: 1–10.
- Luo Y, Kataoka Y, Ostinelli EG, Cipriani A, Furukawa TA. National prescription patterns of antidepressants in the treatment of adults with major depression in the US between 1996 and 2015: a population representative survey based analysis. Front Psychiatry 2020; 11: 35.
- Kappelmann N, Rein M, Fietz J, et al. Psychotherapy or medication for depression? Using individual symptom meta-analyses to derive a symptom-oriented therapy (SOrT) metric for a personalised psychiatry. BMC Med 2020; 18: 170.
- Xu C, Kim TT, Kirsch I, Plöderl M, Amsterdam JD, Pigott HE. Restoring STARD: a reanalysis of drug-switch therapy after failed SSRI treatment using patient-level data with fidelity to the original STARD research protocol. medRxiv 2025; published online Feb 12. https://doi.org/10.1101/2025.02.10.25321991 (preprint).
- Simon GE, Cruz M, Boggs JM, Beck A, Shortreed SM, Coley RY. Predicting outcomes of antidepressant treatment in community practice settings. Psychiatr Serv 2024; 75: 419–26.
- Athreya AP, Brückl T, Binder EB, et al. Prediction of short-term antidepressant response using probabilistic graphical models with replication across multiple drugs and treatment settings. Neuropsychopharmacology 2021; 46: 1272–82.
- Kishi T, Ikuta T, Sakuma K, et al. Antidepressants for the treatment of adults with major depressive disorder in the maintenance phase: a systematic review and network meta-analysis. Mol Psychiatry 2023; 28: 402–09.
- Zaccoletti D, Mosconi C, Gastaldon C, et al. Comparison of antidepressant deprescribing strategies in individuals with clinically remitted depression: a systematic review and network meta-analysis. Lancet Psychiatry 2026; 13: 24–36.
- Henssler J, Schmidt Y, Schmidt U, Schwarzer G, Bschor T, Baethge C. Incidence of antidepressant discontinuation symptoms: a systematic review and meta-analysis. Lancet Psychiatry 2024; 11: 526–35.
- Andrade C. Relative efficacy and acceptability of antidepressant drugs in adults with major depressive disorder: commentary on a network meta-analysis. J Clin Psychiatry 2018; 79: 3331.
- Abdoli N, Salari N, Darvishi N, et al. The global prevalence of major depressive disorder (MDD) among the elderly: a systematic review and meta-analysis. Neurosci Biobehav Rev 2022; 132: 1067–73.
- Devita M, Rossella DS, Adele R, et al. Recognizing depression in the elderly: practical guidance and challenges for clinical management. Neuropsychiatr Dis Treat 2022; 18: 2867–80.
- Motrico E, Moreno-Peral P, Uriko K, et al. Clinical practice guidelines with recommendations for peripartum depression: a European systematic review. Acta Psychiatr Scand 2022; 146: 325–39.
- Radoš SN, Akik BK, Žutić M, et al. Diagnosis of peripartum depression disorder: a state-of-the-art approach from the COST Action Riseup-PPD. Compr Psychiatry 2024; 130: 152456.
- Berk M, Köhler-Forsberg O, Turner M, et al. Comorbidity between major depressive disorder and physical diseases: a comprehensive review of epidemiology, mechanisms and management. World Psychiatry 2023; 22: 366–87.
- Kato M, Hori H, Inoue T, et al. Discontinuation of antidepressants after remission with antidepressant medication in major depressive disorder: a systematic review and meta-analysis. Mol Psychiatry 2021; 26: 118–33.
- McAllister-Williams RH, Arango C, Blier P, et al. Reconceptualising treatment-resistant depression as difficult-to-treat depression. Lancet Psychiatry 2021; 8: 14–15.
- Dodd S, Bauer M, Carvalho AF, et al. A clinical approach to treatment resistance in depressed patients: what to do when the usual treatments don’t work well enough? World J Biol Psychiatry 2021; 22: 483–94.
- Oliveira-Maia AJ, Bobrowska A, Constant E, et al. Treatment-resistant depression in real-world clinical practice: a systematic literature review of data from 2012 to 2022. Adv Ther 2024; 41: 34–64.
- Havlik JL, Wahid S, Teopiz KM, McIntyre RS, Krystal JH, Rhee TG. Recent advances in the treatment of treatment-resistant depression: a narrative review of literature published from 2018 to 2023. Curr Psychiatry Rep 2024; 26: 176–213.
- Steffens DC. Treatment-resistant depression in older adults. N Engl J Med 2024; 390: 630–39.
- Lam MK, Lam LT, Butler-Henderson K, et al. Prescribing behavior of antidepressants for depressive disorders: a systematic review. Front Psychiatry 2022; 13: 918040.
- Levinstein MR, Budinich RC, Bonaventura J, Schatzberg AF, Zarate CA Jr, Michaelides M. Redefining ketamine pharmacology for antidepressant action: synergistic NMDA and opioid receptor interactions? Am J Psychiatry 2025; 182: 247–58.
- Su T-P, Li C-T, Lin W-C, et al. A randomized, double-blind, midazolam-controlled trial of low-dose ketamine infusion in patients with treatment-resistant depression and prominent suicidal ideation. Int J Neuropsychopharmacol 2023; 26: 331–39.
- Duman RS, Sanacora G, Krystal JH. Altered connectivity in depression: GABA and glutamate neurotransmitter deficits and reversal by novel treatments. Neuron 2019; 102: 75–90.
- Njenga C, Ramanuj PP, de Magalhães FJC, Pincus HA. New and emerging treatments for major depressive disorder. BMJ 2024; 386: e073823.
- Fountoulakis KN, Saitis A, Schatzberg AF. Esketamine treatment for depression in adults: a PRISMA systematic review and meta-analysis. Am J Psychiatry 2025; 182: 259–75.
- Patterson R, Balan I, Morrow AL, Meltzer-Brody S. Novel neurosteroid therapeutics for post-partum depression: perspectives on clinical trials, program development, active research, and future directions. Neuropsychopharmacology 2024; 49: 67–72.
- Qiu Y, Tao Y, Duan A, et al. Efficacy and tolerability of zuranolone in patients with depression: a meta-analysis of randomized controlled trials. Frontiers Pharmacol 2024; 14: 1334694.
- de Souza MR, Henriques AT, Limberger RP. Medical cannabis regulation: an overview of models around the world with emphasis on the Brazilian scenario. J Cannabis Res 2022; 4: 33.
- Cairns EA, Benson MJ, Bedoya-Pérez MA, et al. Medicinal cannabis for psychiatry-related conditions: an overview of current Australian prescribing. Front Pharmacol 2023; 14: 1142680.
- Berger M, Amminger GP, McGregor IS. Medicinal cannabis for the treatment of anxiety disorders. Aust J Gen Pract 2022; 51: 586–92.
- Mangoo S, Erridge S, Holvey C, et al. Assessment of clinical outcomes of medicinal cannabis therapy for depression: analysis from the UK Medical Cannabis Registry. Expert Rev Neurother 2022; 22: 995–1008.
- Wolinsky D, Mayhugh RE, Surujnarain R, Thrul J, Vandrey R, Strickland JC. Acute and chronic effects of medicinal cannabis use on anxiety and depression in a prospective cohort of patients new to cannabis. J Affect Disord 2025; 390: 119829.
- Nutt D, Crome I, Young AH. Is it now time to prepare psychiatry for a psychedelic future? Br J Psychiatry 2024; 225: 308–10.
- Butlen-Ducuing F, Silva F, Silva I, Balabanov P, Thirstrup S. Applying the EU regulatory framework for the clinical use of psychedelics. Lancet Psychiatry 2025; 12: 7–9.
- Meng C, Guo W, Xiao C, et al. Structural basis for psilocybin biosynthesis. Nat Commun 2025; 16: 2827.
- Goodwin GM, Aaronson ST, Alvarez O, et al. Single-dose psilocybin for a treatment-resistant episode of major depression. N Engl J Med 2022; 387: 1637–48.
- Wolfgang AS, Fonzo GA, Gray JC, et al. MDMA and MDMA-assisted therapy. Am J Psychiatry 2025; 182: 79–103.
- Hellmann-Regen J, Clemens V, Grözinger M, et al. Effect of minocycline on depressive symptoms in patients with treatment-resistant depression: a randomized clinical trial. JAMA Network Open 2022; 5: e2230367.
- Nettis MA, Lombardo G, Hastings C, et al. Augmentation therapy with minocycline in treatment-resistant depression patients with low-grade peripheral inflammation: results from a double-blind randomised clinical trial. Neuropsychopharmacology 2021; 46: 939–48.
- Qiu Y, Duan A, Yin Z, et al. Efficacy and tolerability of minocycline in depressive patients with or without treatment-resistant: a meta-analysis of randomized controlled trials. Frontiers Psychiatry 2023; 14: 1139273.
- Mathé AA, Michaneck M, Berg E, Charney DS, Murrough JW. A randomized controlled trial of intranasal neuropeptide Y in patients with major depressive disorder. Int J Neuropsychopharmacol 2020; 23: 783–90.
- Bai S, Guo W, Feng Y, et al. Efficacy and safety of anti-inflammatory agents for the treatment of major depressive disorder: a systematic review and meta-analysis of randomised controlled trials. J Neurol Neurosurg Psychiatry 2020; 91: 21–32.
- Ferrari S, Mulè S, Parini F, et al. The influence of the gut-brain axis on anxiety and depression: a review of the literature on the use of probiotics. J Tradit Complement Med 2024; 14: 237–55.
- Meng Y, Sun J, Zhang G. Pick fecal microbiota transplantation to enhance therapy for major depressive disorder. Prog Neuropsychopharmacol Biol Psychiatry 2024; 128: 110860.
- Zhang Q, Bi Y, Zhang B, et al. Current landscape of fecal microbiota transplantation in treating depression. Front Immunol 2024; 15: 1416961.
- Chang M, Chang KT, Chang F. Just a gut feeling: faecal microbiota transplant for treatment of depression—a mini-review. J Psychopharmacol 2024; 38: 353–61.
Fig1
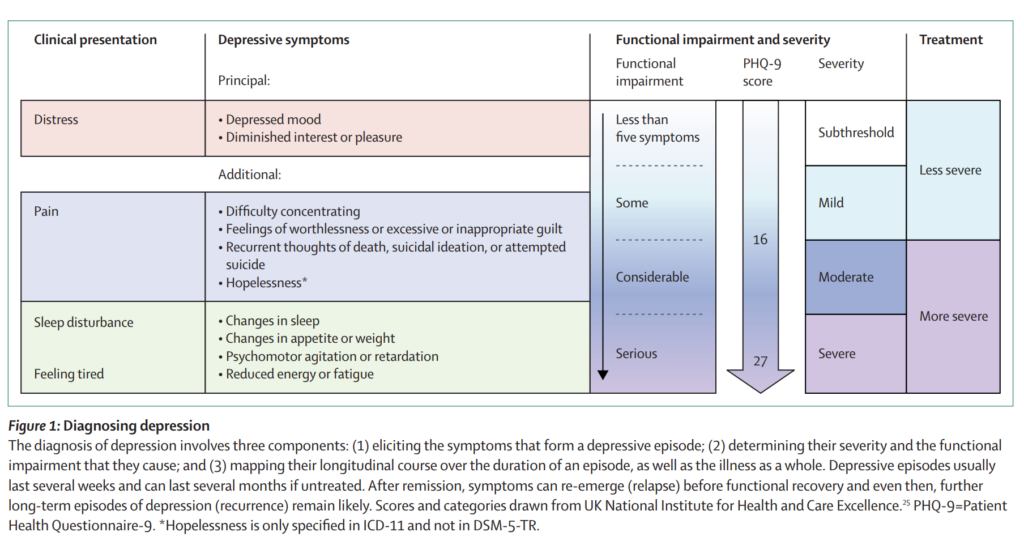
Fig2
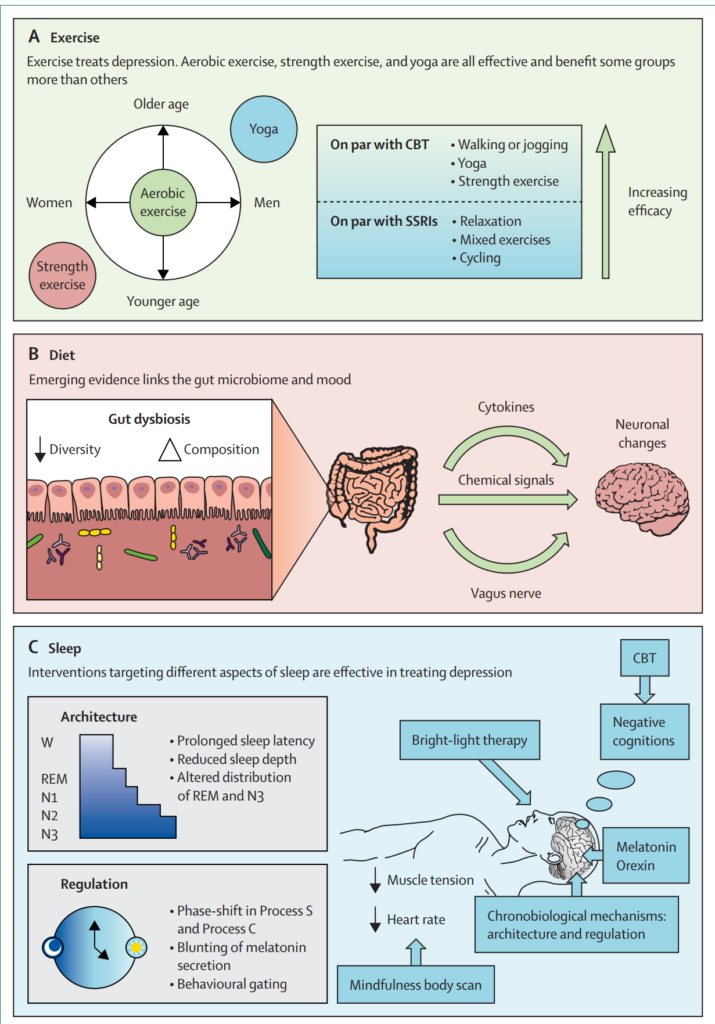
Table1
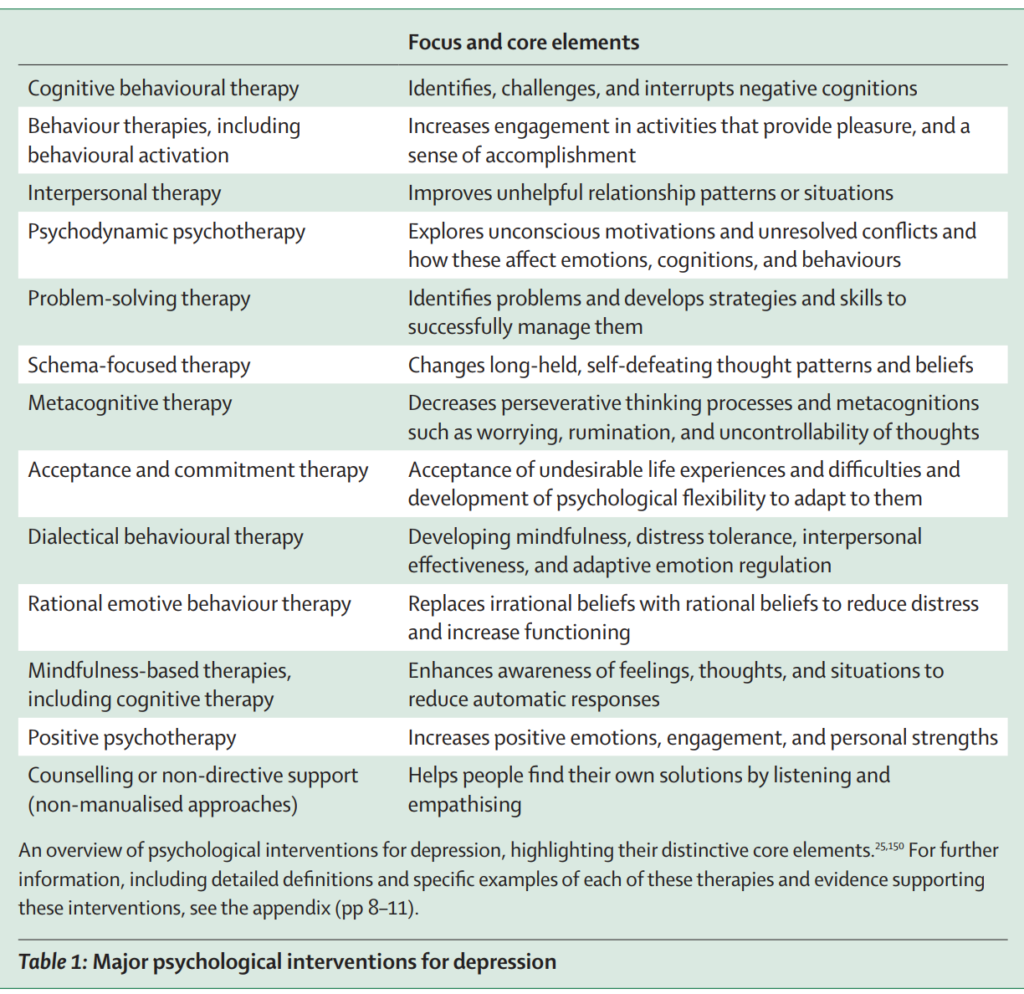
Fig3
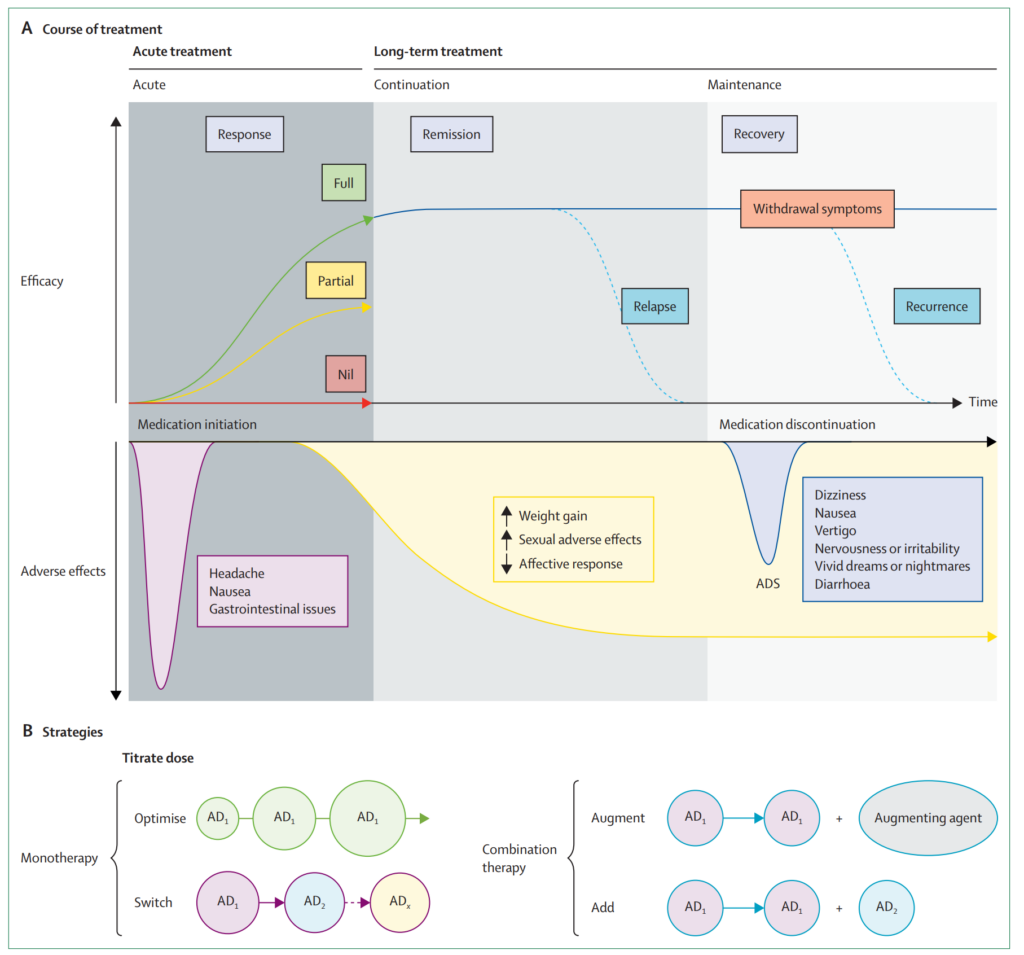
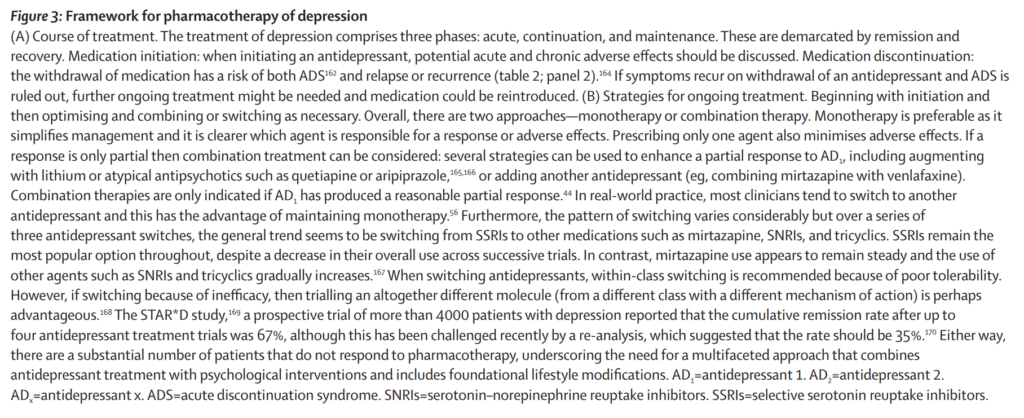
Table2